
OINV Management Advisor
What does your nausea feel like?
Select the description that best matches your symptoms.
Stomach Stasis
I feel full, bloated, or like food isn't moving. I may be constipated.
Dizziness/Motion
I feel dizzy, lightheaded, or sick when I move my head or stand up quickly.
General Nausea
I just feel generally sick to my stomach without dizziness or specific bloating.
Do you have any of these risk factors?
This helps determine safety warnings for certain medications.
Recommended Approach
Imagine you are in pain. Your doctor prescribes a strong painkiller to help you get through the day. But instead of relief, you feel sick to your stomach. You can’t keep food down. This is Opioid-Induced Nausea and Vomiting (OINV), a common and distressing side effect affecting up to one-third of patients taking opioids. It happens to about 20% to 33% of people who take these medications. The problem gets worse when doctors add anti-nausea drugs-called antiemetics-to fix it. If not chosen carefully, these two types of drugs can interact in dangerous ways.
You might think that adding an anti-nausea pill is a simple fix. It isn’t always. Some combinations can slow your breathing, affect your heart rhythm, or trigger a rare but serious condition called serotonin syndrome. Understanding how these drugs work together is crucial for staying safe while managing pain.
Why Opioids Make You Feel Sick
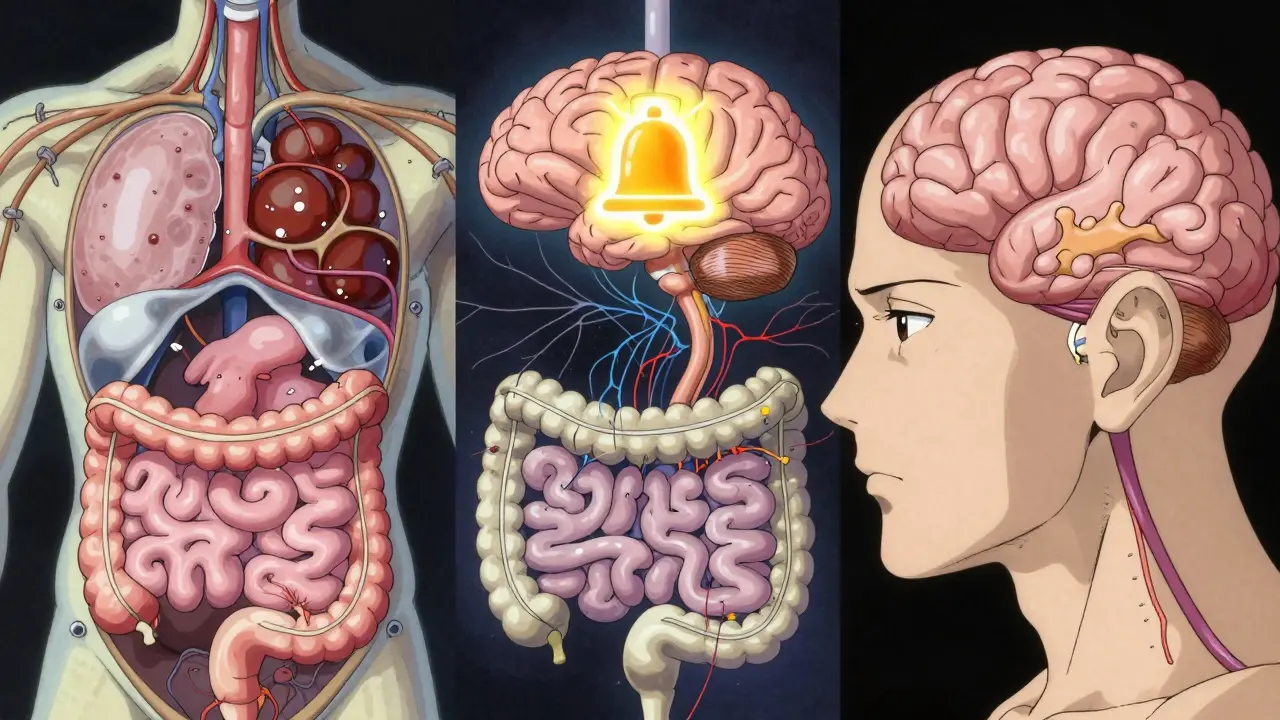
To manage nausea effectively, you first need to understand why it happens. Opioids don’t just block pain signals; they mess with several parts of your body at once. There are three main reasons you feel sick after taking them:
- The Gut Slows Down: Opioids bind to mu-opioid receptors in your digestive tract. This slows down movement (motility). Food sits in your stomach longer than it should. This stagnation sends signals to your brain that make you feel nauseous. It’s the same mechanism that causes constipation.
- The Brain’s Alarm Bell Rings: Deep in your brain is an area called the chemoreceptor trigger zone (CTZ). Opioids stimulate dopamine receptors here. Think of the CTZ as a smoke detector. When opioids hit it, it goes off, telling your brain to vomit to "clear out" what it thinks is poison.
- Your Inner Ear Gets Confused: Opioids can increase sensitivity in your vestibular system. If you stand up quickly or move around, you might feel dizzy or lightheaded. This motion sickness contributes significantly to the overall feeling of nausea.
Good news? For most people, this nausea is temporary. Your body usually builds tolerance to the emetic (vomiting) effects within 3 to 7 days if the dose stays constant. However, waiting it out isn’t always an option, especially if you need to eat or stay hydrated.
Choosing the Right Antiemetic: Mechanisms Matter
Not all anti-nausea drugs work the same way. Picking the right one depends on which of the three mechanisms above is causing your symptoms. Using the wrong type might do nothing-or worse, cause new problems.
| Drug Class | How It Works | Best For | Key Risks |
|---|---|---|---|
| Serotonin Antagonists (e.g., Ondansetron) | Blocks serotonin (5-HT3) receptors in the gut and brain. | General opioid nausea, post-surgery vomiting. | Prolonged QTc interval (heart rhythm issue), constipation. |
| Dopamine Antagonists (e.g., Metoclopramide) | Blocks dopamine in the CTZ; speeds up gut emptying. | Nausea caused by slow digestion. | Movement disorders (tardive dyskinesia), sedation. |
| Antihistamines/Anticholinergics (e.g., Meclizine, Scopolamine) | Calms the vestibular (inner ear) system. | Dizziness, motion sickness, position-related nausea. | Dry mouth, blurred vision, confusion (especially in older adults). |
For example, if your nausea feels like motion sickness when you walk, an antihistamine like meclizine is likely more effective than ondansetron. If you feel full and bloated because your gut has stopped moving, a prokinetic agent like metoclopramide might help-but recent evidence suggests prophylactic use (taking it before symptoms start) may not be very effective for intravenous opioids.
The Hidden Dangers: Drug Interactions
The biggest risk in treating OINV isn’t just the side effects of the antiemetic itself-it’s how it interacts with the opioid and other medications you might be taking. Two major interaction risks stand out.
1. Serotonin Syndrome
This is a potentially life-threatening condition caused by too much serotonin in your brain. Certain opioids, particularly tramadol and methadone, have serotonergic properties. If you combine these with certain antiemetics or other drugs, you stack the deck against yourself.
The FDA has issued specific warnings about this. Mixing opioids with antidepressants (like SSRIs or SNRIs) or migraine medications (triptans) can trigger serotonin syndrome. Symptoms include agitation, hallucinations, rapid heart rate, fever, muscle rigidity, and loss of coordination. While less common with standard antiemetics, the risk increases if you are on multiple central nervous system (CNS) active drugs.
2. Cardiac Risks: The QTc Interval
Both ondansetron and droperidol carry black box warnings from the FDA. Why? They can prolong the QTc interval on an electrocardiogram (ECG). A prolonged QTc interval can lead to a dangerous heart rhythm called torsades de pointes, which can stop your heart.
If you already have heart conditions, low potassium or magnesium levels, or are taking other drugs that affect heart rhythm (like some antibiotics or antifungals), using these antiemetics requires caution. Always inform your doctor about your full medical history.
Best Practices for Safe Management
So, how do you handle this safely? Here is a practical approach based on current clinical guidelines, including the 2022 CDC Clinical Practice Guideline for Prescribing Opioids.
- Start Low, Go Slow: Never jump into high doses. Start with the lowest effective dose of the opioid. Titrate up slowly over days or weeks. This allows your body to adjust and reduces the shock to your GI tract and brain.
- Educate Before You Treat: Doctors should warn patients that nausea is common and often temporary. Knowing that it will likely pass in 3-7 days can reduce anxiety, which itself can worsen nausea.
- Target the Cause: Don’t just grab any anti-nausea drug. Ask yourself: Is it dizziness? Use an antihistamine. Is it stomach stasis? Consider a prokinetic. Is it general chemical irritation? A serotonin antagonist might be best.
- Consider Opioid Rotation: If one opioid makes you violently ill despite antiemetics, switch to a different one. Individual variability is huge. For instance, tapentadol has a lower risk of nausea compared to oxycodone, which in turn is safer than oxymorphone regarding GI side effects per pharmacokinetic studies.
- Avoid Unnecessary Prophylaxis: Unless you have a history of severe vomiting, routine pre-treatment with antiemetics isn’t always necessary. Reactive treatment (treating when it happens) is often sufficient and avoids unnecessary drug exposure.
Special Considerations for Older Adults
Older adults are more vulnerable to both opioid side effects and antiemetic interactions. Their bodies metabolize drugs slower. They are also more sensitive to anticholinergic effects (dry mouth, confusion, falls). The Beers Criteria, a list of potentially inappropriate medications for older adults, flags many antihistamines and dopamine antagonists as risky due to cognitive side effects.
For elderly patients, non-pharmacological strategies are key. Small, frequent meals. Ginger supplements (which have mild anti-nausea properties). Hydration. And strict adherence to the "start low" principle. If an antiemetic is absolutely needed, short courses of low-dose ondansetron are often preferred over long-term use of metoclopramide due to the latter’s risk of movement disorders.
When to Seek Help
While nausea is common, it’s not something you should just endure. Contact your healthcare provider if:
- Vomiting prevents you from keeping down fluids or pain medication.
- You experience signs of dehydration (dark urine, dizziness, dry mouth).
- You notice heart palpitations or fainting (possible cardiac interaction).
- You develop confusion, agitation, or muscle stiffness (possible serotonin syndrome).
Effective pain management shouldn’t come at the cost of your well-being. By understanding the mechanics of OINV and the risks of antiemetic interactions, you can work with your doctor to find a balance that keeps you comfortable and safe.
How long does opioid-induced nausea last?
For most patients, opioid-induced nausea is temporary. Tolerance to the emetic effects typically develops within 3 to 7 days of starting a constant dose. If nausea persists beyond this window, it may indicate an underlying issue like severe constipation or an incorrect medication choice, requiring a review by your doctor.
Can I take ondansetron with my opioid prescription?
Yes, ondansetron is commonly prescribed for opioid-induced nausea. However, it carries a risk of prolonging the QTc interval (a heart rhythm measure). If you have existing heart conditions or take other medications that affect heart rhythm, consult your doctor first. It is generally safe for short-term use in healthy individuals.
What is serotonin syndrome, and how do opioids cause it?
Serotonin syndrome is a serious reaction to excess serotonin in the brain. Some opioids, like tramadol and methadone, increase serotonin levels. Combining these with other serotonergic drugs (such as certain antidepressants, migraine meds, or some antiemetics) can trigger this condition. Symptoms include confusion, rapid heart rate, high blood pressure, and dilated pupils. Seek immediate medical attention if these occur.
Which opioid causes the least nausea?
Individual responses vary greatly, but studies suggest that tapentadol has a lower risk of gastrointestinal side effects like nausea and constipation compared to oxycodone or oxymorphone. Fentanyl patches also tend to cause less GI distress because they bypass the gut initially. If one opioid causes severe nausea, ask your doctor about rotating to a different class.
Is it better to prevent nausea or treat it after it starts?
Recent Cochrane reviews suggest that prophylactic (preventative) use of certain antiemetics like metoclopramide for IV opioids may not significantly reduce nausea risk. For oral opioids, starting with a low dose and increasing slowly is the best prevention. Treating nausea reactively with targeted antiemetics is often more effective and avoids unnecessary drug exposure unless you have a history of severe vomiting.









